92. Психодинамика бессознательного в случае психосоматической болезни: предварительные методологические соображения. Г. Аммон (92. Psychodynamics of the Unconscious in the Case of Psychosomatic Illness: Methodological Preconsiderations. Gunter Ammon)
Deutsche Akademie fur Psychoanalyse. Lehr- und Forschungsinstitut fur Dynamische Psychiatrie und Gruppendynamik. BRD
Psychoanalytic understanding of psychosomatic illnesses is unthinkable without a theory of the unconscious. Therefore, it follows logically within the historic development of psychoanalysis beginning with Freud, that the dynamics of the unconscious and the manifestations of psychosomatic phenomena have always been metapsychologically closely correlated. Notably for Freud and many of his successors this did not so much imply extensive comprehension of psychosomatic problems, but rather the formulations of the theoretical pre-conditions, necessary to this initial understanding, which they achieved. This situation is primarily due to the absence of a universally recognized scientific concept of the unconscious, both in psychology and in the foundations of psychoanalytic theory. The term "unconscious" embraces a wide spectrum of diverging scientific views, although, generally speaking, one ought to point out that in investigating psychosomatic disturbances, both psychoanalysis and the Soviet school of psychology fundamentally take into account unconscious factors in the evolving stages of psychosomatics, despite terminological and objective differences.
If it is possible, however, to accept this common guideline, a theoretical dimension of the unconscious in the field of psychosomatics must be postulated in order to achieve an understanding of the term "unconscious" itself which in a specific way covers psychic phenomena as well as the problems of physical stages of development and physical conditions. In the course of my report this will be investigated more closely. Freud's discovery of the dynamics of the unconscious resulted in the primary understanding of previously unknown fields of the patient's psychic experience and behavior and could be first understood in the course of practical treatment.
Freud was looking for a method which could make the pathology of the patient clear to the patient himself, i. e. clear to the self-perception of the personality. Psychopathological symptoms, whose rigidity is supported by the dynamics of unconscious forces (denied by the patient) are to be integrated into the patient's ego. Through conscious realization these symptoms then become therapeutically reversible. This insight forced Freud continually to construct the concept of the ego in relation to a theory of the unconscious. In his paper "The Ego and the Id" of 1923 he shows that psychic processes, in particular the processes of ego-formation, cannot be reduced to conscious elements alone; the ego is in large parts unconscious. In the same paper Freud supplements this with a further idea specifying the relationship between the psychically qualified ego and its somatic equivalent: the body-ego.
The content of the unconscious is related to the libido, to the drives which are combined in the "id" (the person's instinctual sphere) and the instincts as such are accessible to the somatic region. Instincts are the psychic representatives of continually flowing, inner-somatic sources of stimulation. Thus the ego is directly related to the psychosomatic organism as a whole, looked at in reference to the libido theory. Therefore the unconscious ego-elements represent the somatic region within the ego itself. Some of Freud's investigative ideas on psychosomatics in his earlier works, primarily concern themselves with the structure of hysterical conversion symptoms as special forms of repression achievements. They can be incorporated into this concept of a metapsychological relationship between ego-formation and body-ego based on a theory of the unconscious. The transition from the psychic level into the somatic innervation is carried out as hysterical conversion in those cases where incompatible ideas of instinctual impulses are rendered harmless by means of channelling the whole excitation into physical form. The physical symptom is. the somatic representative of such an incompatible idea which in the process of neurotic repression of instincts is blocked.
It is true that Freud's theory of conversion and his theory of the instinctual dynamics of the unconscious have proven productive in the past. Thus orthodox psychoanalysis to this very day largely builds its theoretical foundations on an understanding of them. I, on the other hand, share the opinion of several Soviet psychologists (Ph. Bassin, Kon and others) that the mutual influence of psychic agencies and their conflictingly arrested antagonism, confined exclusively along intrapsychic lines of instinctual dynamics, can cover sufficiently neither the sociological nor the biological conditions which today must be considered to play a major role in the explanation of the pathogenesis of psychosomatic illnesses. My theory of ego-identity and body-ego-identity forms the basis of my concept of psychosomatic illnesses. In this theory I have treated the unconscious in the framework of the psychodynamic unit of the personality. As such I have conceived of it, firstly, as a group of primarily given psychophysiological ego-roots which are simultaneously present while the individual grows up, and secondly, as the unit of primary group-relationships which interpersonally manifest themselves within the symbiosis between mother and child. Ego-roots and the dynamics of the primary group together form the internalized elements which, each in their own way, comprise the unconscious structural conditions of the ego- and body-ego-identity. Therefore the unconscious as such does not exist in the sense that one could show its existence as an empirical entity by way of experimental reconstructions. Here, too, I agree with Bassin's ideas. On the contrary, the unconscious is part of a type of formulation of hypothesis which is indispensable in psychoanalytic theory and practice. The task of therapeutic work must then be to verify, correct and modify. Psychoanalysis is, above all a science of therapy. Therefore the way in which psychoanalytic science formulates its concepts leads- to theorems, which can be falsified by observable, clinical phenomena and. which are subject to the reality-test of feedbacks, whose methodologically indispensable prerequisites they are.
My research in the field of psychoanalytical and group psychotherapeutical situations, as well as in the clinical field of psychiatric practice have shown that the unconscious psychodynamics of the principal psychosomatic syndrome specifically refers to the total unity of the individual personal identity. The previously mentioned pathological manifestations in the form of a psychosomatic syndrome can only be comprehended in the differentiated steps of reflection in terms of a reciprocal effect between the psychobiological, hereditary capacities of the ego and those internalized primary-group-relationships of the ego-identity. The psychophysiological elements in the constitution of the ego and the body-ego as well as the structure of primary and secondary groups are part of the context of historical and social conditions. These historical and social constellations leave their mark upon the unconscious group- and personality dynamics.
For these reasons, I have related the therapeutical techniques of treatment for psychosomatic illnesses with a combined methodology, which connects the pathological deformations of the ego and the body-ego-structures to the pathogenesis of their simultaneously corresponding group dynamical relations, in which the psychosomatic lived. The emerging phenomena of transference and resistance in the context of individual and group situations form a diagnostic criterion for the therapeutically relevant insights into the destroyed identity of the psychosomatic's unconsciously carried psycho- and group dynamic relations. Therefore in view of my theoretical conception of the unconscious, psychoanalytic group therapy is in theory and in clinical practice a central scientific and therapeutic tool for the treatment and investigation of psychosomatic illnesses.
In that which follows, I would like to proceed along the lines of psychotherapeutic study of the psychosomatic syndrome. I hope to illustrate the psychogenetic structure and dynamics in the personality of the psychosomatic, as well as interpret and delineate the psychosomatic's pathological attempts at restitution through the enaction of his symptoms.
The Psychosomatically III
The application concerning a specific psychotherapeutic technique has to be related to the understanding of the nature of the illness. I find that there are certain psychological signs indicative of psychosomatic diseases: for these patients there seems to be no connection between their somatic symptoms and the difficulties they have in their life. Sometimes they appear to have al-most schizoid traits, but they become alive as soon as they can draw full attention to their somatic symptoms. They can talk endlessly about their somatic diseases, as if only this activity could make them feel alive. To this extent, one might call them quite narcissistic. They demand attention and care, presenting themselves extremely in need of symbiotic dependency. In this dependency - should the need not be fulfilled - they appear depressed and with a demanding attitude towards environment, but without interest for persons and things.
This behaviour is of course just a superficial form of a deep-lying structure which, generally, I would call the psychosomatic patient's mode of life. In order to understand the conflicting behavior of dependency and isolation and its psychodynamic relation to the psychosomatic symptom, especially for the purpose of developing therapeutical techniques, it is important to reflect upon the earliest anamnestic information gathered about the patient and his symptom as well as psychosomatic symptomatology in general.
The Development of the Ego and of Body-Ego-Identity in Early Mother-Child Relationships
The conditions which lead to psychosomatic diseases are to be found in specific experiences of early childhood. The earlier the disturbance of the primary development takes place, the graver will be the consequences. This becomes obvious when we consider the conditions required to furnish the child with an optimum frame of reference for the formation of basic functions and abilities. During the first period of life, a child does not experience itself as separated from the mother. It does not differentiate between the internal and external, between self and non-self, between ego and non-ego. The mother is experienced as a part of its own body, the body itself having no clear boundaries as yet; the child is not yet able to perceive its own functions. Mother and child represent a psychosomatic unit. They live in a dyadic symbiosis. Apart from providing the material basis for existence, it is the task of this symbiosis to produce a post-natal climate (food and care) in which the child, through the close, emotional and physical contact with the mother, can register and experience its own needs and body reactions and will thus become aware of its own body.
This interpersonal situation between mother and child contains the primary conditions necessary for the child to experience itself. The archaic feeling of existence that the mother first transmits to the child on the level of tactile and olfactory contact has already at this genetical stage a definite and unique "configuration" (Lichtenstein, 1961), which is shaped essentially by the experience and behavior of the mother towards her child. This specific and unique configuration of "primal identity" which the child experiences in the mirror of motherly affection must in my opinion be seen as the forerunner and model for the ego-boundary, which the child in close physical contact with the mother gradually builds up as the ego-boundary. Thus the "world of the primieval cavern" (Spitz, 1955) is not only a necessary condition for the faculties of the ego and the functional psychic and physical structures. Primarily it is also a place in which the earliest, primary process demarcations of the child's ego-identity take place; in the course of this process, the ontogenetic frame of ego and body-ego boundaries originates.
This guarantees the development of the ego-functions in the framework of the psycho-physical units of human personality.
The "Gap in the Ego" and the Psychosomatic Symptom
Therefore the manifestations of psychic and somatic disorders invaribaly indicate that there are disturbances within the interpersonal and group processes which, during the early childhood relation to the mother, form the basis for the psychosomatic development of the growing individual. Pathological alterations of the simultaneous psychosomatic development - a term that best describes the dyadic structure of communication of the primary group- consequently produce ruptures in the psychosomatic organization in the personality of the child itself. Thus the group aspect is closely related to the understanding of ego and body-ego-formation; therefore the forms of early childhood interaction and communication with the closest object, the mother, are essential elements in a theory of ego and bodv-ego-identity; at the same time they are a decisive factor in the understanding of how manifest psychosomatic symptoms originate and how one ought to proceed methodologically in the flexible therapeutical applications of analytical group therapy.
In that which follows, I would first like to discuss the structural relationship between psychosomatic pathology (which the general practitioner is daily-confronted with) and primary processes in the history of mother and child. In its earliest stage of development the child depends on the mother's presence as an auxiliary ego so that through suitable reactions to its needs in dealing with the child she will start to establish its body boundaries. If the mother is not able to play this role, the child can suffer severe damage during this period of first development. By this I mean the narcissistic deficit which will sustain itself throughout the subsequent stages of development. Therefore within the symbiosis between mother and child the interpersonal process plays a- decisive part in the formation of the child's body-ego (Fig. 1).
In my work with patients reacting psychosomatically, I have observed again and again that during childhood the mothers of these patients reacted with particular helplessness when it came to active and aggressive reactions. They interpreted any spontaneuos expression of life as an offence to their own- narcissism. In cases where these children tried alternatively to gain their mother's attention through compensating motor activities, these signals were negated, not recognized and prohibited. The consequences: immobility, hyperactivity and pathological transformation of the originally constructive aggression into destruction which then is directed against the child's body. The person reacting psychosomatically says "no" to his own self. Already in childhood this "no" appears in the form of organ-pathological reactions and as a direct expression of disintegration of the body-ego-identity.
It then becomes clear that the development of the basic body functions and forms of reaction is dependent upon the all-important affective physical communication between mother and child in early symbiosis, during which the child internalizes the mother's attitude and behavior and, in doing so, shapes a body-ego which - by means of the earliest ego-boundary, i. e. the body-ego-boundary - permits an initial differentiation between the internal and external. On the basis of this, an ego-sensation of bodily existence can take shape and the necessary conditions for an active interaction can be instituted. This manifests itself in the development and differentiation of ego-functions. At the same time the child understands the inability to experience as an anxiety of existential abandonment - frequently in the form of open hostile rejection or simple indifference. This happens especially in cases when the mother, because of her own particular need-structure, prematurely detaches herself from the child. The child is then forced to develop defence mechanisms - an energy-consuming means to re-establishment of harmony with its mother. For the psychosomatic adult this sudden desertion remains a traumatic experience of early childhood; subsequently all ego-forces are tied down in the attempt to prevent the corresponding anxieties from recurring.
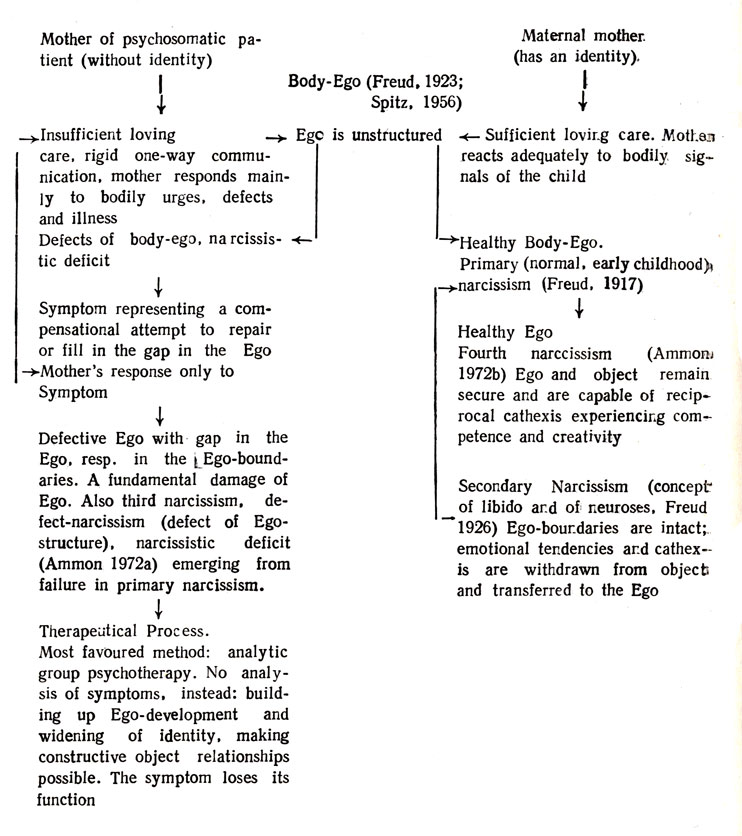
Figure 1
Furthermore, because of this state of desertion the weak ego-boundaries of the child are in danger of being flooded by inner and outer non-ego-content which can lead to the disintegration of the entire ego-feeling. Flexible ego-demarcation and a free expression of the ego towards the inner and the outer are replaced by compulsive mechanisms in order to fend off the danger of ego-disintegration. Through this, however, those realms of experience are cut off because the mother obstructed or extremely controlled the child's expression of central ego-functions, constructive aggression and creativity. The reality that corresponds to these experiences must be negated, leaving, so to say, "white spots" on the map of the ego, zones in which the child's ego remains incapable of internal and external experience because these situations remain linked to an archaic anxiety of existence. In this way the structural deficit in the development of the ego-boundary or as I have called it, "gap in the Ego", occurs and the realms of experience thus afflicted cannot be incorporated in subsequent development.
The psychopathological symptoms resulting from this - the field of psychosomatic illness included - was described by me as spectrum of archaic ego-diseases; they are generally characterized by a lack of ability to demarcate the identity; patients reacting psychosomatically usually cling in a symbiotic way to undifferentiated real and remembered objects which they perceive to be devouring and deserting simultaneously. I interpret this type of psychodynamics caused by such a "symbiotic complex", as an attempt to arrive at an ego-demarcation and accordingly independent communication with oneself and others by plugging the symptom into the gap in the ego (see Ammon, 1971, 1972 a, b; 1973). So the psychosomatic disease must be seen as an expression of a structural ego-illness. This means that during the stage of body-ego development the patient suffered damage in the form of a traumatic defect to his ego-roots, thereafter making the departure from the dependency on the disturbed symbiosis impossible for him. Since the ego-feeling and reality-testing of this patient could not be fully developed because of this given life-history, he subsequently often produces an overadjustment to the demands of the external world or an isolated state of separating from many realms of life. The psychosomatic reacts to every-day experience in professional, social and individual situations by escaping into a false identity. Because of this huge existential anxiety the sick person tries to escape from the actual, real question of "who am I?" by replacing it with the symptom-oriented question of "what is the matter with me, what am I suffering from?". He incessantly seeks to answer this question by constantly turning to physicians and medical institutions. In other words, the question of his own identity is replaced by the question about the symptom which has to cover the deficits in the broken identity. Here the symptom represents the internalized mother of early childhood who blocked the normal behavior of the child and was capable of responding maternally only when her child was ill.
In the symbiotic primary process the child identifies itself with the mother's inability 1o relate. In the phase of archaic identification with the mother the child's ego learns (besides the ability to demarcate its ego) to observe and to internalize the mother's modes of being, especially those of a controlling or abandoning mother.
Therefore it becomes understandable that an adult psychosomatic patient observes his body functions and slight changes in its usual functioning with a fascinated, anxious or severe kind of exactitude; this reflects his relation to his mother who withdrew from him; correspondingly he observes his body as if it did not belong to him, just in the same way as he had perceived his mother: absent and primarily constituting no part of him during the early phase of symbiosis.
In these dynamics we often find two contradictory reactions tied together which are characteristic of the ambivalence, in the personality of patients suffering from ego-deficiencies, particularly those with psychosomatic illnesses. On the one hand, the psychosomatic symptom is a representative of destructive aggression resulting from the internalization of the hostile maternal aspects. On the other hand it expresses the patient's own hostility, which fluctuates symbiotically between dependency and animosity.
In my works on aggression I have always differentiated this destructive aggression from a constructive one, which I regard as an early manifestation of primary autonomy of the ego and as a central ego-function. My experience in the field of psycho- and group dynamic relations between ego-identity, aggression and groups led to an understanding of destructive aggression as a historically formed result of certain primary and secondary group-constellations, and not as a descendant phenomenon of an innate drive of destruction. I think, the latter is just a speculation, and other scientists, like Ph. Bassin, are of the same opinion. Destructive aggression is a result of a pathological transformation of a primordial constructive aggression that expresses itself in a healthy curiosity when approaching human beings and things. The conflictual blocking and mutilation of the primary ego-function of aggression in the development of a child result mainly from reduced communication in primary groups that are incapable of responding to basic needs; their pathological communication becoming internalized in the structure of ego-formation in the psychodynamics of their individuals.
A good example for such an internalisation of pathology is given in the case of psychosomatics. They draw their destructive aggressions onto themselves, this being expressed in their symptoms. At the same time they direct these aggressions towards the internalized parts of the bad object in the body-ego, reflecting the early mother-child communication. The dynamics of destructive aggression also shows, according to my experience from a very large number on cases, that in correlation with the isolation of feelings within the frame of the psychosomatic symptom another emotional isolation takes place: the isolation of the patient arid his inability to enjoy positive relations (personal and in groups). Psychosomatic patients show a general, structural inability to establish contact with groups, and thus live accordingly in "dead" relationships. From this we should conclude, that in planning effective therapeutic situations one should always consider having heterogeneous groups. We have had good results, for instance, when putting "genuine" psychosomaties with patients suffering from conversion, such as in hysteria. Psychosomatic patients (in a selection from over 100 patients' reports known to me) show a tendency toward strong alternation between needs for dependency and a sudden break of relationship, leading to extreme anxiety of separation and abandonment. For their therapy in groups it is thus very important to provide stabilizing factors of communication, for example by joining them with patients with neurotical conversion symptoms. In conversion hysteria the psychodynamical damage has occurred at a later age, namely in the oedipal phase, in which the rivalry between parent and child of the same sex has led to phantasies of abandonment, resulting from projection of hostility on the rival-parent. Within the process of identity formation in the group the analytical group situation enables the interception of the psychosomatic's narcissistic trauma and the integration of this trauma into the strong and flexible ego-boundaries of the group, thus bringing it under therapeutical control.
The Symptom as a Hostile Super-Ego
The intrapsychic balance of the psychosomatic is always under a stress reaching much deeper into the archaic levels of ego development in the pre- and post-natal concomitants than that of a conversion neurotic. The illness- producing family shows up as a pathogenous trauma which stays with the patient throughout his subsequent life-history. By force of repetitive compulsion this trauma leads to a destructive structure within the patient's ego itself: a hostile and cruel super-ego which is characteristic of the psychosomatic.
In this connection the psychosomatic symptom has a special function in which it fulfills two requirements which the severe super-ego insists upon. It transforms the body-ego feeling into something that is foreign to and cut off from the ego. This then - in its symptomatic form - is consciously recognized as being inferior and repulsive (the splitting off of the failing and traumatizing family situation during childhood becomes apparent here). At the same time the symptom fulfills an extremely compensatory function. In exchange for his illness the psychosomatic manages to get attention and care (independent of the control and compulsions of his super-ego), from the surrounding group and from a society which through its general practitioners and clinical practice reacts positively to the manifest psychosomatic symptomatics. On the other hand psychosonatics react with rejection and lack of understanding in cases of mental illness.
The Shifting of Somatic Symptoms
In my opinion it is, therefore, important to draw attention to the close relationship between psychopathology and psychosomatics. We can observe impressive changes and shifts of symptoms within as well as between the two dimensions (see Fig. 2).
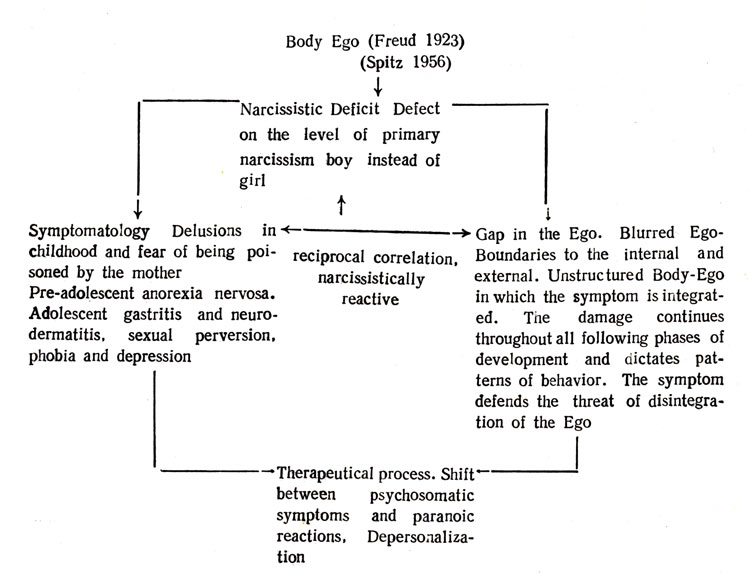
Figure 2
For instance, a neurodermatitis can turn into a bronchial asthma which in turn can change into a phenomenon like obesity. Within the process of symptom-shifting, psychosomatic disturbances can pass over into pathological manifestations which are characteristic of psychotic reactions, and these again are in many ways interrelated with other forms of ego-diseases on a fluctuating spectrum. The dynamics of psychosomatic pathology can therefore be illustrated through a comparison with other phenomena of ego-diseases, especially since, within the phenomenology of archaic personality and body-ego disorders, a shifting of symptoms can be observed that prove the relation in their equivalent structures. I would like first to emphasize the point that there are decisive differences between this archaic symptomatology and a neurotic one, although neurotics also tend to produce symptom-shiftings. The neurotic converts his unconscious instinctual conflict mainly into conflicts between his intrapsychic agencies. They then appear in dreams, compulsive activities, and - somatically seen - in conversion symptoms. The neurotic patient experiences his symptom as alien to the ego and as an impairment of his ability to deal with his surrounding environment. The symptomatical transformation of an intrapsychic conflict impairs within the neurotic an essentially developed and demarcated ego; the object-relationship to reality and to the body-self are mainly intact. The outer objects can be clearly separated from the inner ones in the phantasies and dreams of the patient. However, the contact to external reality has disappeared almost totally in the case of the archaic ego-illnesses, particularly in the case of the psychotic reactions, in the context in which psychosomatic structures must be looked at. The separation of external and internal reality has broken down; the patient's behavior and realm of experience are completely governed by imagined feelings of unlimited power or anxieties of annihilation which are experienced as real. Therefore the patient reacting psychotically projects his dreams, anxieties and repetition compulsions upon reality; in his acute states the patient with an ego-defect experiences the total loss of reality and ego.
The psychosomatic reaction occupies an intermediary position between the psychotic loss of object and the neurotic conversion symptoms, a position which in its psychodynamics corresponds to the so-called borderline syndromes which also include sexual perversion.
Psychosomatics and the Spectrum of Archaic Ego-Illnesses
In psychosis the boundary between ego and non-ego, internal and external, is broken down, and the ego is flooded by nonintegrated, unconscious content which - in the pathological sense- tries to restrain psychotic disintegration. The psychosomatic symptom on the other hand forms an equivalent for the psychotic disintegration of the ego whose unconsciously self-destructive dynamics are locked inside more or less extended, somatic disorders; by this means the psychosomatic symptomatics, i. e. a partial disintegration of the body-ego, can be instrumental in preserving the intactness of the remaining ego- and body-ego regions.
This interpretation corresponds to the results of empirical research going as far back as C. G. Jung (1907) and Dreyfuβ (1908). During the period of an organic illness psychotically ill patients remain free of psychotic reactions. On the basis of similar observations Kutemeyer (1953) was able to develop his theory of the "equivalent character" of psychosomatic illness. In connection with my own research (Ammon, 1972), I reported on a patient who during childhood had constantly suffered from agonizing skin diseases - eczemas, purulent skin-rashes, primarily on the face and hands. During puberty he contracted a severe case of bronchial asthma, which lasted more than 10 years. When through autogenic training the asthma attacks stopped completely, he experienced a state of psychosis-like depression which led him to seek out the help of the psychoanalyst. During analytic sessions he suffered states of extreme depression which he termed "asthma without asthma" (Ammon, 1972). The disrupted symbiotic communication of the child with its mother depicts the psychosomatic symptom as the internalized bad object and in this sense becomes the expression of a certain form of defense which uses the child's own body since no other form of separation from the bad object in early childhood was possible.
The Unconscious Parts of the Body-Ego
This discussion of pathogenesis and the possibilities of therapy in the case of psychosomatic symptoms is based on the presupposition of metapsychological relationships of the ego and the body, as I have pointed out already. I would like to return to this point now with particular respect to the scientific work of the problem of the unconscious in Soviet psychology. As was shown earlier, the dynamics of psychosomatics implies a concept of the individual's body-reality which itself shows the characteristics of the ego-identity from the ontogenetically earliest beginnings. As far back as 1923 Freud was able to specify the body-ego rudimentary, primary ego. Later this idea was taken up and expanded upon, mainly by E. Glover and R. Spitz. Spitz considered the concept of the neuro-psychological ego-nuclei as components of the ego whose prototypes are mostly innate psychological functions, passed on phylogenetically as well as in hereditary behavior patterns. The body-ego which combines the ego- nuclei, is seen by Spitz as being an archaic forerunner of the ego, which like all living things, possesses a synthesizing and integrating tendency. These ego-nuclei, formed directly after birth, are autonomous. Starting from this point, the transition from the psychic to the somatic sphere is accomplished. This biogenetic development is accompanied by mother-child interactions in which the alleged primary physiological ego-nuclei are supplied with psychic content as a result of cathexis by libido and then are transformed into psychic ego-nuclei. Spitz can therefore assume psychic ego-representatives of neuro-physiologically given ego-functions. The prototypes of the psychic ego-nuclei are to be found in the physiological functions and in the somatic behavior of the rudimentary ego.
In my work on psychosomatics, I have pointed out (contrary to Spitz), that the formation of psychic ego-boundaries and the formation of the ego identity become possible already in the first stages of mother-child-symbiosis. I would like to place the anthropogenetic priority in the neurophysiological dimension of rudimentary ego-nuclei that leads to a later synthesized psychic totality of the ego-identity with a dynamic parallelism between the neurophysiological growth of the individual and his psychogenetic ego-development. Already the act of smiling, which Spitz has discussed, should be interpreted as a first indication of ego-boundaries being formed, permitting the child in the presence of the mother to feel its own existence. The premises of the ego-identity are then, in my opinion, not the alleged fragmentary physiological ego-nuclei, but rather the primal identity which the child experiences under the protection of the symbiosis with the mother. In the dyadic "world of the primal cavern" (Spitz) the child also forms and develops this ego-identity and its boundaries into body-ego boundaries. Therefore, I assert, contrary to Spitz, that the body-ego, which develops during the various stages of mother-child-symbiosis, must from the beginning be regarded under the aspect of communication and identity-development. Disorders during the archaic body-ego-development stages must therefore always be seen as ego-identity-disorders as well, which, psychodynamically speaking, represent impairments of the ability to experience within the realm of interpersonal object-relationships.
At this point, I see the possibility to proceed to a conception of the unconscious which, through the term itself, would in principle convey the concept of ego- and body-ego-identity. In my opinion, Spitz directed his theory of neuro-physiological ego-nuclei away from this aspect of identity. In the course of my research, I have come to understand that the aspect of ego- and body-ego-identity from the very beginning is an integral part wherever the somatic and psychic regions converge. It plays a part in the primary behavioral modes of the interpersonal relationships between mother and child as well as in the cathexis of body-ego-elements and also in psycho- and group dynamics which manifest themselves in the earliest ego-elements. For the following reasons this controversy between Spitz and myself might be of interest particularly to Soviet psychologists.
Initially it appears as if one could combine Spitz's and my theoretical differences into a framework with the help of Leontyev's materialistic theory on the principles of the psychic development of the child. Spitz can define the unconscious in a neuro-physiological way, though his definition does not' contain the concept of identity, whilst Leontyev works on the expressions of the unconscious and a theory of personality according to which the unconscious is a totality of the phylo- and ontogenetic history of an individual, in addition to his socially preformed process of acquisition.
In the development of the individual these factors represent the sphere1 of a differentiated objectivity; the unconscious turned objective, so to say. Also the genesis of the abilities and functions of the individual must be seen within the materialistically conceived dialectic content of history. They represent products of complicated processes of action and operationalism through which the child - on the matrix of objective (i. e. biological, social, cultural etc.) conditions - develops its organs and their psychic equivalents in an experimental manner. Leontyev, however, obviously places more importance on social rather than biological factors. He is then confronted with the difficult problem of the anatomical-physiological basis of the individual functions that have been acquired on a socio-historical level. Because of certain scientific-materialistic presuppositions it is impossible for Leontyev to assume the existence of abilities and functions which could not be attributed to a specialized organ, analogous to them. At this point, I see a similarity with my concept of the unconscious quality of ego-functions. Leontyev sees them as developments from genetic and functional constellations of an innate psychological mechanism and individual experiences within the historical attempts of the individual at learning and acquisition respective to phylo- and ontogenesis. Leontyev avoids, as I do, explaining psychic manifestations (the ego-unctions, i. e. although he does not use an explicit ego-concept) as a result of physiological processes, as Spitz has done in his theory of the ego-nuclei. One-way causality of physiological basis and psychic phenomenon is replaced, analogous to my conception, by the processual interdependence of the anatomical-physiological substrate with the dynamics of the psychic region which I have formulated in the dialectics of the ego- and body-ego-identity. Leontyev sees the psychic factor not as something that is idealistically separated from the objective world, but rather as an element within a context in which psychic factors and physio-biological phenomena of equal original importance constitute the objectivity of real life and society. The unconscious cannot be reduced to physiology, instead it is inherent to both dimensions which, according to my theory, find their expression in a steady development of ego. In my conception therefore, the relationship between the neuro-physiological ego-nuclei and the central ego-functions methodologically shows the characteristics of an inversive dialectic. The neuro-physiological structure of the ego-nuclei like ego-feeling, perception, motility, tactile-optical compounds etc. is always based upon the psychodynamic correlate of ego-identity with its relationships to objective reality. The central constructive ego-functions, like aggression, creativity, and the ego-regulation can also not be thought of without their neuro-physiological correlates.
Nor can the unconscious physiologically be reduced to the reservoir of repressed drive-potential, as Bassin has pointed out. At this point, I can fully agree with Bassin's criticism of Freud and orthodox Freudianism which have given recognition to the unconscious only within the conceptual framework of functional antagonisms of libidinal, intrapsychic systems. That is why, until today, the Freudian theory of psychosomatic syndromes has hardly transcended the drive-dynamically oriented concept of conversions. I share Bassin's point of view that the unconscious is not a complex which can be isolated within the limits of intramental processes. Through my research and clinical experience, however, I was able to break through the total isolation of the unconscious by orthodox psychoanalysis and individual- and drive-psychology.
The methodological position, that unconscious processes should be understood in a dialectical intertwining of physiologically laid ego-nuclei with the central manifestations of primary ego-autonomy, allows me to examine the group dynamical and socio-cultural backgrounds of psychopathology. Positions that are only based on drive-psychology misjudge not only the relation of ego-identity and physiology, but also split the ego and body-ego-processes into genetical, dispositional origins and interpersonal dimensions, which in my theory are linked in the concept of the unconscious.
My additional attempt to demonstrate my understanding of psychosomatics, as well as the pathologies in the whole spectrum of ego-diseases, is based on a theory of identity that integrates both factors of the psychogenetical .and neurophysiological. This theory of identity of the ego and body-ego necessarily requires in therapeutical work an ability to deal with the unconscious balance between individual psychodynamics and the process within the group and at the same time cannot deny the correlative medium of ego-identity with its historical and trans-individual character.
References
1. Ammon, Gunter (1971): The Psychosomatic Symptom in its Relation to Ego and Group Dynamics. In: Promotions of the I. Int. Congress Int. College Psychosom. (Med. Gua- delajara, Mexico)
- (1972): Zur Genese und Struktur psychosomatischer Symptome unter Berucksichtigung psychoanalytischer Technik. In: Dyn. Psychiat. (5) 223-251.
- (1973): Dynamische Psychiatrie - Grundlagen und Probleme einer Reform der Psychiatrie (Darmstadt: Luchterhand)
- (1974): Psychoanalyse und Psychosomatik (Munchen: R. Piper)
2. Bassine Ph. (1973): Le probleme de L'Inconscient (Moskau: Editions Mir).
3. Budilowa J. A. (1975): Philosophische Probleme in der sowjetischen Psychologie (Berlin: Deutscher Verlag der Wissenschaften).
4. Dreyfuβ G. (1908): Nervose Dyspepsien. Zit. nach: Kutemeyer, W. (1953): Korpergeschehen und Psychose (Stuttgart: Enke).
5. Freud S. (1923): Das Ich und das Es. Ges. W. Bd. XIII (London: Imago).
6. Jung C. G. (1907): Uber die Psychologie der Dementia Praecox (Halle: Marhold).
7. Kon J. S. (1971): Soziologie der Pers?nlichkeit (K?ln: Pahl-Rugenstein).
8. Kutemeyer W. (1953): Korpergeschehen und Psychose (Stuttgart: Enke).
9. Leontjew A. N. (1973) : Probleme der Entwicklung des Psychischen (Frankfurt: Fischer Athenaum).
10. Lichtenstein H. (1961): Identity and sexuality. A study of interrelationship in men. In: J. Am. Psychoanal. Assn. (9)..
11. Spitz R. A. (1955): Die Urhohle: Zur Genese der Wahrnehmung und ihrer Rolle in der psychoanalytischen Theorie. In: Psyche (IX) 641-667.
|
ПОИСК:
|
При копировании материалов проекта обязательно ставить активную ссылку на страницу источник:
http://psychologylib.ru/ 'Библиотека по психологии'